|
In June 2024, I received a message from a fellow CDI physician advisor. His colleagues were arguing that “Type 2 NSTEMI” wasn’t a legitimate clinical entity. I had seen similar debates by cardiologists on social media, making us both pause and question our understanding. Were we wrong? Should we stop using the term “Type 2 NSTEMI” altogether?
Let’s take a step back. How do we define a myocardial infarction? According to the 4th Universal Definition of Myocardial Infarction (4UDMI), two key criteria must be met:
- Evidence of acute myocardial injury
- Signs or symptoms of ischemia
Both criteria are required for a diagnosis of MI.
Breaking Down the Definitions
- Acute Myocardial Injury: This occurs when cardiac troponin levels rise above the 99th percentile upper reference limit (URL). A rise and/or fall in troponin levels indicates an acute injury, while an unchanging pattern suggests chronic injury.
- Evidence of Ischemia: The 4UDMI outlines four potential indicators, any one of which suffices:
- Symptoms of acute myocardial ischemia (e.g., angina or anginal equivalents)
- New ischemic ECG changes
- Development of pathological Q waves
- Imaging evidence of new loss of viable myocardium or regional wall motion abnormality consistent with ischemia
If both criteria are met, then the diagnosis of MI is supported. The distinction between Type 1 and Type 2 MI depends on the underlying etiology:
- Type 1 MI results from atherothrombotic coronary artery disease, often triggered by plaque disruption (rupture or erosion).
- Type 2 MI stems from an oxygen supply-demand mismatch.
Where Does “NSTEMI” Fit In?
The terms STEMI (ST-segment elevation myocardial infarction) and NSTEMI (non ST-segment elevation myocardial infarction) describe ECG findings rather than MI types. Neither ECG finding is unique to a type. In fact, ST-elevation can occur in 3–24% of Type 2 MIs according to the 4UDMI. Finally, to address the initial concern, can you meet the criteria for a myocardial infarction with supply-demand mismatch? Absolutely. If there’s no ST-elevation, it’s technically a Type 2 NSTEMI—but here’s the catch:
The 4UDMI doesn’t use the term “Type 2 NSTEMI.” It only uses “Type 2 MI.” So, even though it’s an accurate descriptor, should we use “Type 2 NSTEMI” in documentation? The answer is no—and not just to avoid irking cardiologists. There are important quality reporting implications at play.
The CMS Readmission Program
CMS tracks 30-day unplanned readmissions for acute myocardial infarctions (AMIs) under the Hospital Readmissions Reduction Program (HRRP). This cohort isn’t based on DRG assignment but rather on the principal diagnosis code of the index admission.
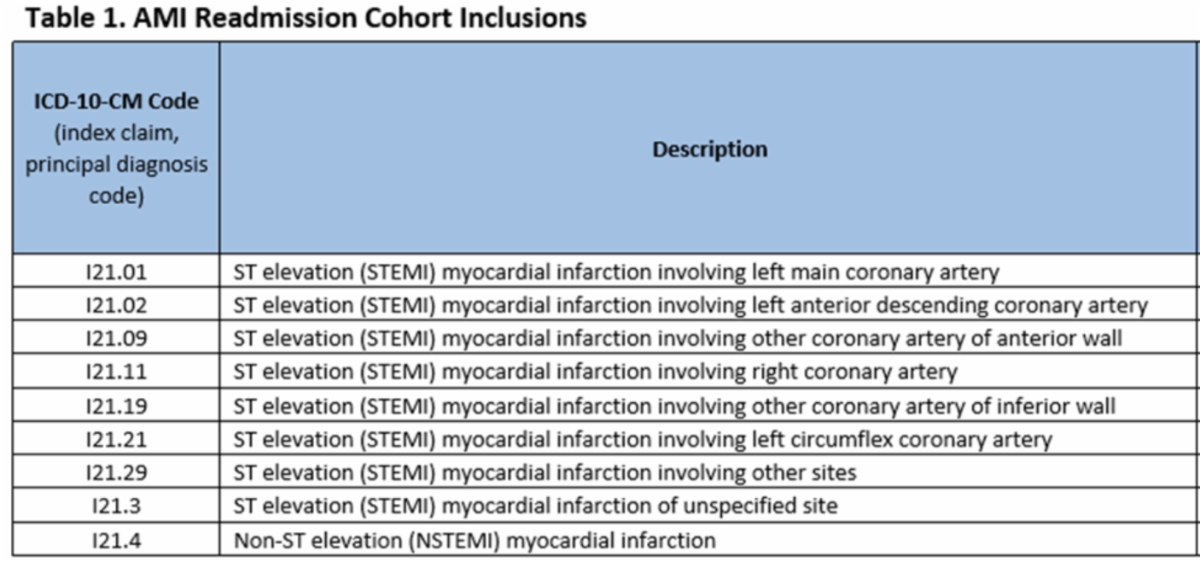
Before we get to those codes, note that there was a coding clinic that advised the coding of Type 2 MI. Coding Clinic Fourth Quarter page 62 states, “Type 2 myocardial infarction is assigned to code I21.A1, Myocardial infarction Type 2 with the underlying cause coded first, if applicable… If a Type 2 AMI is described as NSTEMI or STEMI, only assign code I21.A1. Codes I21.01-I21.4 should only be assigned for Type 1 AMIs.”
With that in mind, the codes used in the CMS 30-day AMI readmission cohort are as below:
|